For Mrs. Mu, the mother of an 8-year-old girl, her thoughts are different
from doctors. Shen thinks for patients and their families, sometimes they
are vulnerable groups compared to doctors and other medical staff in some
cases.
She told about the experience of her daughter who has been taken to a
hospital in Zhejiang Province after feeling collywobbles for a long period.
“I didn’t mean to find fault, but I was really annoyed by what the doctor
did at that time,” said Mrs. Mu.
Facing the tough and emergency situation, anxious parents chose to register
a relatively more expensive specialist to prove the accuracy of diagnosis.
Their daughter was diagnosed with a kind of stomach disease.
After two weeks of observation and taking medicine, the girl did not take
a turn for the better, so the parents took the girl to the other doctor,
Chen, to check. But Chen refused to add a quota contemporarily for the
girl despite she was her patient. At the same time, she agreed to add a
quota for the other patients. In addition, the doctor rebuffed the demand
of parents that she would explain the reason for the symptom.
Mrs. Mu was enraged by the situation and complained to the relative bureau
of the hospital. However, her complaint received no response. The security
department of the hospital told Mrs. Mu that the doctor had the right to
decide if she would add a quota for someone. “But I think she didn’t treat
my daughter equally,” said Mrs. Mu, “since she chose to add a quota for
the other patient while my daughter was waiting there.”
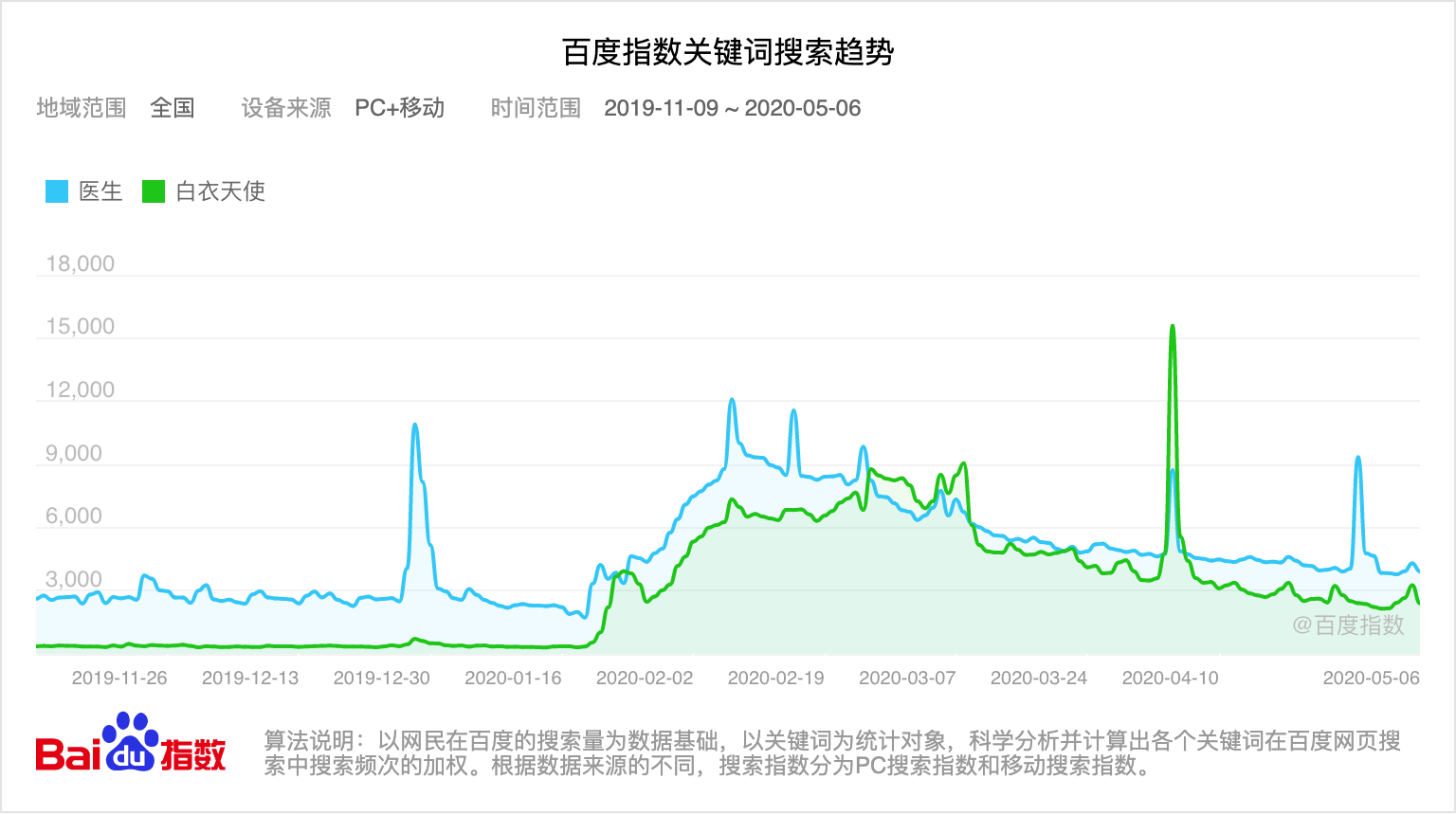
Liu is another person who complained about her experience of seeking medical
advice during the outbreak of COVID-19.
She has suffered from slightly breathing difficulties for a long time.
In February, after the outbreak of COVID-19 took a turn for the better,
she went to a tertiary hospital in Dalian and booked a doctor of respiratory
medicine department.
After waiting for about 1 hour, she entered the inquiry room and saw the
doctor. She described her symptoms to the doctor detailedly, but only received
a query from the doctor.
“You are really young. I don’t think you may have some illnesses.” said
the doctor. But she did not elaborate on the reason for her symptoms. “Maybe
you just lack practice.” The doctor thought for a while and made a conjecture
without any substantive suggestions.
Under Liu’s repeated requests, the doctor agreed Liu do chest radiography.
Another two hours of waiting passes, when Liu brought the chest radiography
and reported back to the doctor, the doctor did not even check the X-ray
film.
“She just read the report sketchily and concluded that there’s nothing
wrong with my respiratory system.” said Liu, “I was a little annoyed not
because I didn’t get any effective diagnosis, but it is because she didn’t
treat me with any graveness. She concluded that it was my anxiety that
made me uncomfortable without checking my chest radiography.”
Liu still suffers from chest distress and shortness of breath until now.
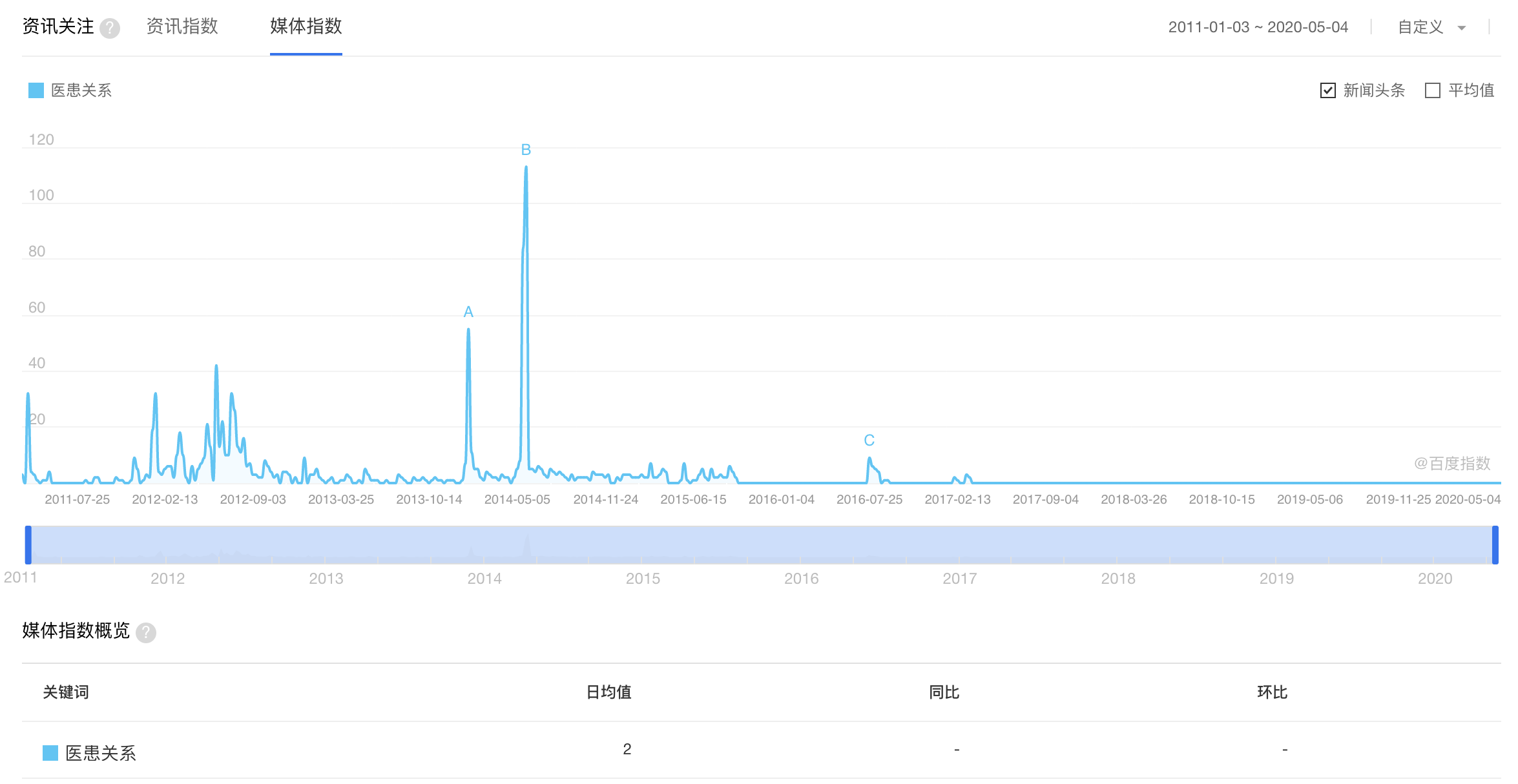
Cases mentioned above are what sometimes could happen during and after
the treatment. Two different systems of thoughts exist in doctors’ and
patients’ minds, which cause contradictions between them.
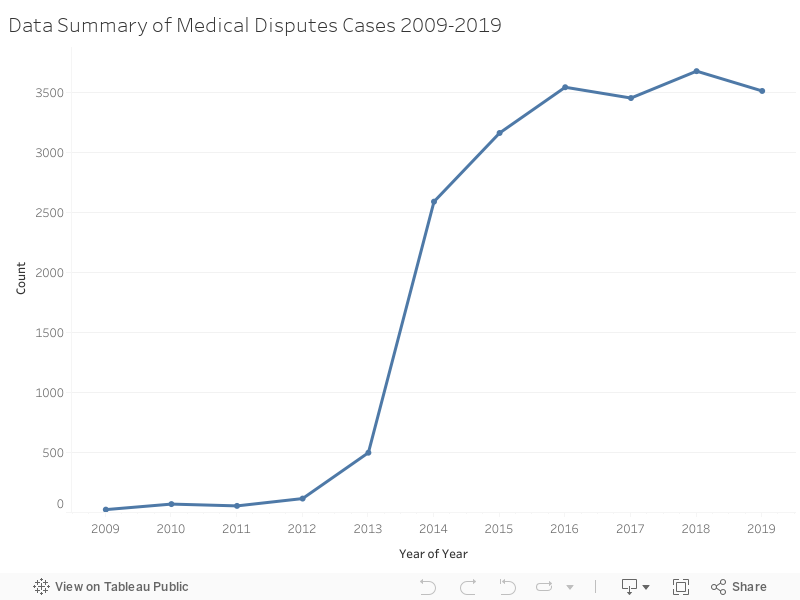
Medical dispute cases emerge after incidents happen and patients usually
have two solutions, legal approach, and compounding.